 Tweet
Tweet
Re: Humilin N vs. Vetsulin
Glad your post worked the second time around Al. Happy to see you respond to the cushings questions too. This is really is an amazing site where both the K9D & K9Cushings work closely together.
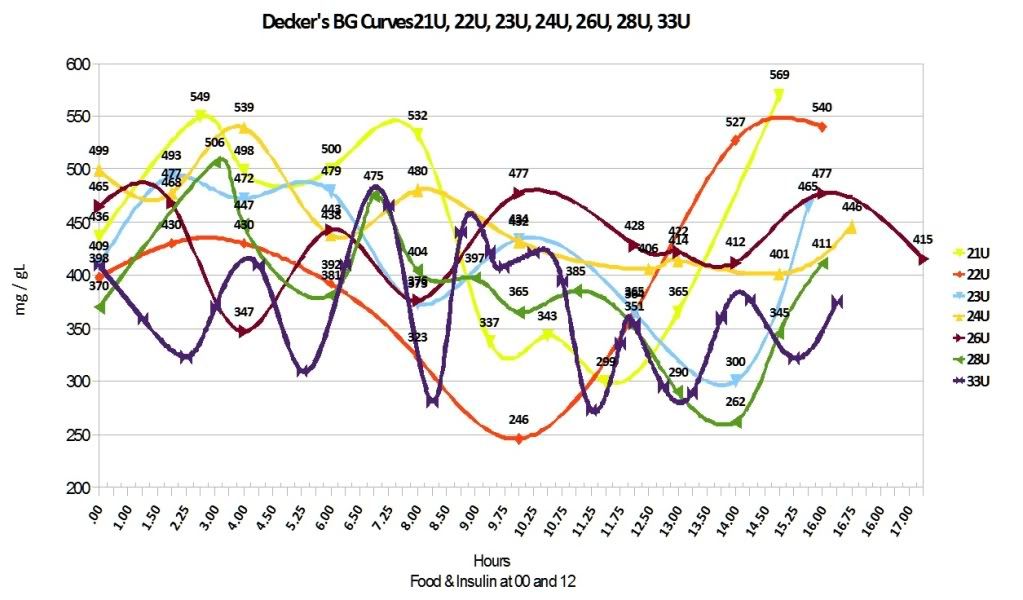
Decker did bounce around a lot on the NPH. His curves looked like a roller coaster ride gone bad.
Here is a picture:
You can have a full thyroid panel run through Dr. Dodd's by having your GP vet do the blood draw and then you mail the sample to hemopet. Dr. Dodd's recommended the Thryoid Profile 5 for Decker.
Here is a link to the form:
https://labordatenbank.com/cake/hemo...s/hemopet_form
Here is a link to some FAQs on the Hemopet site:
http://www.hemopet.org/index.php?opt...=faq&Itemid=27
Here is Dr. Dodd's email: hemopet@hotmail.com
I would recommend emailing her if you have any questions regarding her testing. Might be worth asking her about the steroids ahead of time because I think I remember reading that steroids can impact thyroid testing. I'm sure she'd be able to give you much more detailed information. She has always been great about responding to me. Only one time, when she was out of the country, was there more than a two day delay in response time.
We overnighted the sample because of the summer temps but there is no need to overnight them. Cost us around 25.00 for vet blood draw, 80.00 for Hemopet testing and 30.00 for overnight mailing. There was around a two day turn around time. The results were emailed to me and my vet was copied on them as I had asked. Dr. Dodd's takes into account a dogs breed, age, and other factors - thus Decker's 'case specific' reading was based on his specific information.
Will follow up later to address some of your other questions.
Glad your post worked the second time around Al. Happy to see you respond to the cushings questions too. This is really is an amazing site where both the K9D & K9Cushings work closely together.
Decker did bounce around a lot on the NPH. His curves looked like a roller coaster ride gone bad.
Here is a picture:
You can have a full thyroid panel run through Dr. Dodd's by having your GP vet do the blood draw and then you mail the sample to hemopet. Dr. Dodd's recommended the Thryoid Profile 5 for Decker.
Here is a link to the form:
https://labordatenbank.com/cake/hemo...s/hemopet_form
Here is a link to some FAQs on the Hemopet site:
http://www.hemopet.org/index.php?opt...=faq&Itemid=27
Here is Dr. Dodd's email: hemopet@hotmail.com
I would recommend emailing her if you have any questions regarding her testing. Might be worth asking her about the steroids ahead of time because I think I remember reading that steroids can impact thyroid testing. I'm sure she'd be able to give you much more detailed information. She has always been great about responding to me. Only one time, when she was out of the country, was there more than a two day delay in response time.
We overnighted the sample because of the summer temps but there is no need to overnight them. Cost us around 25.00 for vet blood draw, 80.00 for Hemopet testing and 30.00 for overnight mailing. There was around a two day turn around time. The results were emailed to me and my vet was copied on them as I had asked. Dr. Dodd's takes into account a dogs breed, age, and other factors - thus Decker's 'case specific' reading was based on his specific information.
Will follow up later to address some of your other questions.
 , I haven't been able to catch up on your thread, but on a quick glance it doesn't look like you have gotten an aswer to whether or not you should join at the k9cushings site. Yes, please join that group as it will easier for you to get all of their members input.
, I haven't been able to catch up on your thread, but on a quick glance it doesn't look like you have gotten an aswer to whether or not you should join at the k9cushings site. Yes, please join that group as it will easier for you to get all of their members input. -- Pointer/Lab | 75 lbs | 11.5 yrs |diagnosed 10/2012 | A-Typical Cushings (Adrenal Exhaustion) since 2008 treated w/small doses of steroids | home test w/meter | boiled chicken breasts/thighs - no skin/bones, frozen green beans, and oatmeal
-- Pointer/Lab | 75 lbs | 11.5 yrs |diagnosed 10/2012 | A-Typical Cushings (Adrenal Exhaustion) since 2008 treated w/small doses of steroids | home test w/meter | boiled chicken breasts/thighs - no skin/bones, frozen green beans, and oatmeal
 The prescription hydrocortisone has a half life much shorter than Medrol but again, I don't know anything about NHC. Hydrocortisone's half life is 8 to 12 hours while Medrol is 18 to 36 hours. When switching over or weaning off a drug, you have to be very, very careful to do it right; otherwise, you place the dog at risk. Even in smaller doses of Medrol taken long term, you have to assume that the adrenal glands are asleep at the wheel and you must take the difference in half life into consideration when transitioning Otherwise, you could underdose or overdose. My fear with a natural supplement is that you are underdosing and Mini is going through withdrawal or her adrenal glands are not yet producing enough cortisol. Did your vet give you specific instructions on how to transition to NHC? If not, I highly recommend that you contact your vet asap.
The prescription hydrocortisone has a half life much shorter than Medrol but again, I don't know anything about NHC. Hydrocortisone's half life is 8 to 12 hours while Medrol is 18 to 36 hours. When switching over or weaning off a drug, you have to be very, very careful to do it right; otherwise, you place the dog at risk. Even in smaller doses of Medrol taken long term, you have to assume that the adrenal glands are asleep at the wheel and you must take the difference in half life into consideration when transitioning Otherwise, you could underdose or overdose. My fear with a natural supplement is that you are underdosing and Mini is going through withdrawal or her adrenal glands are not yet producing enough cortisol. Did your vet give you specific instructions on how to transition to NHC? If not, I highly recommend that you contact your vet asap.
Comment